Retake
A15) Thin stools and unintentional weight loss
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with nausea and vomiting.
- Review the DDx considerations in a patient with nausea and vomiting.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with nausea and vomiting.
History
A 70-year-old male presents to the emergency department due to progressive abdominal distension, nausea, vomiting, and an inability to pass gas. He also mentions a change in bowel habits, reporting that he has been passing thin stools for the past 5 months, despite attempts to manage it with over-the-counter laxatives and stool softeners. His most recent colonoscopy was performed 10 years ago and showed no abnormal findings. The patient further unintentional weight loss of 40 pounds over the last 6 months and experiences dizziness upon standing. He has experienced several falls the past few weeks with resultant back pain secondary to the dizziness. The patient reports a surgical history of a L4-L5 posterior lumbar fusion.
Physical Exam
Vital signs: Blood Pressure (BP) 110/75 mmHg, Heart Rate (HR) 69 beats per minute, Respiratory Rate (RR) 18 breaths per minute, Temperature 97.2°F, Oxygen Saturation (SpO2) 97% on room air.
Abdominal Examination: The abdomen is distended and tympanic on percussion. There is minimal tenderness to palpation. There is no rebound tenderness or guarding.
Rectal Examination: Although no overt blood is observed on the glove during the digital rectal exam, the fecal occult blood test (FOBT) is positive.
Neuro: Point tenderness over superior lumbar spine. Intact strength and sensation in all extremities.
Labs
Hemoglobin (Hb): 8.2 g/dL (Normal range: 13.5-17.5 g/dL in men).
Carcinoembryonic Antigen (CEA): 12 ng/mL (Normal range: <3 ng/mL).
Provisional Diagnosis
Select the Dx you believe is most appropriate
Considering the patient's history of thin stools and weight loss, the physical exam findings of a palpable rectal mass, the lab findings of anemia and elevated CEA, and the positive fecal occult blood test, the most appropriate diagnosis is colorectal cancer. The recent onset of nausea, vomiting, inability to pass gas, and abdominal distension could likely be secondary to a bowel obstruction caused by this colorectal cancer.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
In this patient, there are no signs of bowel ischemia, such as rebound tenderness, rigidity, or guarding, which would indicate a need for emergent surgery. Furthermore, the patient is hemodynamically stable. Therefore, although the patient requires urgent evaluation and management, immediate workup and management may not be necessary.
First Imaging Study
What is the first imaging study you will order?
In patients with suspected high-grade bowel obstruction, the most appropriate initial imaging modality is a CT scan of the abdomen and pelvis. CT scans are accurate in identifying the presence and cause of obstruction, and detecting the presence of complications, such as strangulation and ischemia.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
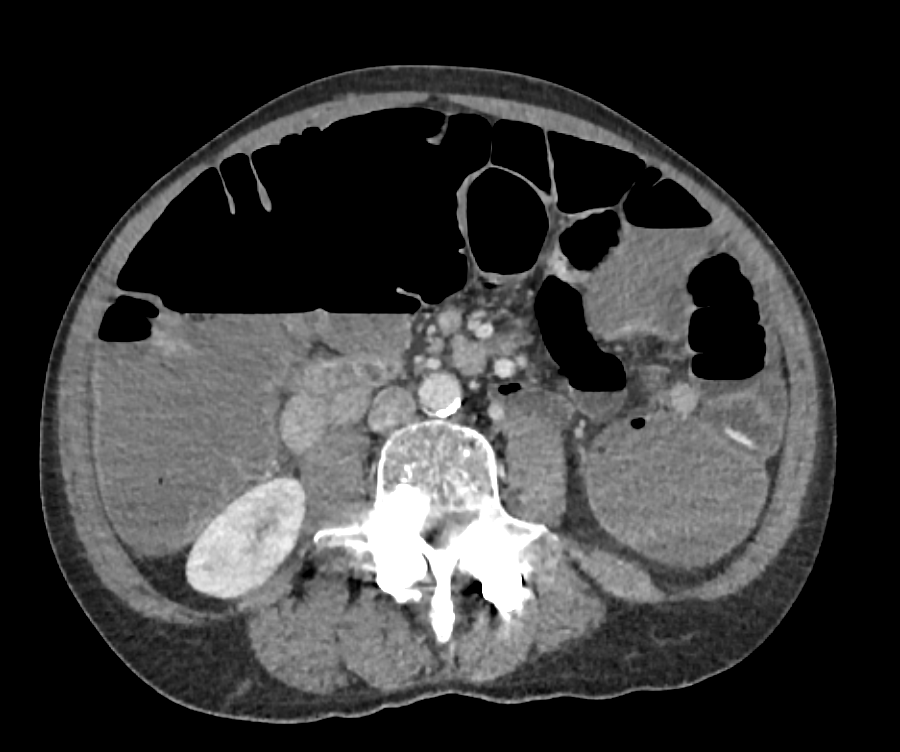
CT of the abdomen and pelvis with IV Contrast
What part of the bowel is distended?
The large bowel is significantly distended. The haustal markings indicate that this distended structure is the large bowel.
What finding is present in the rectum?
The rectum demonstrates circumferential bowel wall thickening and stricture formation. This is a characteristic finding in colorectal cancer, commonly referred to as an "apple core" lesion.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
If additional imaging is needed, both transrectal ultrasound and MRI can offer precise local staging, thus aiding in surgical planning and assessing resectability following neoadjuvant treatment, if applicable. These images are not shown in this case.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient, presenting with a rectal lesion characterized by eccentric wall thickening, an "apple-core" appearance of the rectum, obstruction, and associated lymphadenopathy, is most likely suffering from rectal adenocarcinoma.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
The 70-year-old male patient presents with symptoms indicative of a bowel obstruction secondary to colorectal cancer, including abdominal distension, thin stools, and significant weight loss. The anemia, elevated CEA, and positive fecal occult blood test support this diagnosis. Imaging confirms large bowel distension resulting from a colonic obstruction with thickening and stricturing at the high rectum. The presence of mesorectal adenopathy suggests potential lymph node involvement. An L1 compression fracture, likely related to recent falls from orthostatic hypotension due to symptomatic anemia, is also noted. Our plan is to initiate a multidisciplinary oncology team consultation. The patient's care may include a biopsy of the lesion, and surgery, radiation, and chemotherapy, depending on the disease extent and patient's overall health status. In the interim, the patient should undergo placement of an NG tube and receive antiemetics and analgesics. For the L1 fracture, a conservative approach with pain management, physical therapy, and potential bracing should be considered.
Lessons Learned:
- Colorectal cancer may be discovered by routine screening, can present with suspicious signs and symptoms, or may present with acute presentations due to peritonitis or as in this case, intestinal obstruction.
- Radiological studies may reveal distinct features such as eccentric wall thickening, the characteristic "apple-core" appearance, obstruction, and concurrent lymphadenopathy.
- A transrectal ultrasound and MRI of the pelvis are the imaging modalities of choice for locoregional staging.
Socioeconomic Factors: Various modifiable risk factors are associated with colorectal cancer, such as a diet rich in processed or red meat, a sedentary lifestyle, obesity, tobacco use, and substantial alcohol consumption. Proactive lifestyle adjustments may reduce colorectal cancer risk.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}